GORE® VIABAHN® Device family
Case Studies
Join the next generation of care in the treatment of aortoiliac occlusive disease
Treating severe aortoiliac occlusive disease (AIOD) at the aortic bifurcation
GORE® VIABAHN® VBX Balloon Expandable Endoprosthesis
Case submitted by Jean Panneton, M.D.
Norfolk, Virginia
Challenge
- 73-year-old female presented with bilateral buttock, thigh, calf and foot claudication.
- Femoral pulses not palpable bilaterally.
- Relevant patient history:
- Breast cancer, hypertension, hyperlipidemia
- Former heavy smoker
- Baseline ankle-brachial index (ABI) = 0.49 bilaterally.

Figure 1. Aortoiliac occlusive disease at aortic bifurcation.
Procedure
- Angiography revealed severe calcification of the bilateral common iliac arteries with anterior tibial and posterior tibial run-off to the right foot and posterior tibial run-off to the left foot (TASC II D lesion).
- Deployed two 6 x 39 mm GORE® VIABAHN® VBX Balloon Expandable Endoprostheses (VBX Stent Graft) simultaneously in a kissing stent technique (Figure 2).
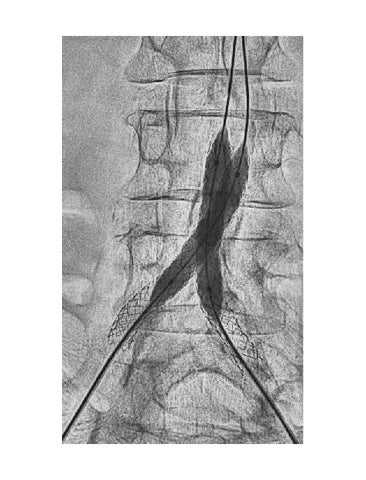
- Follow-up angiogram showed successful deployment and brisk distal run-off (Figure 3).
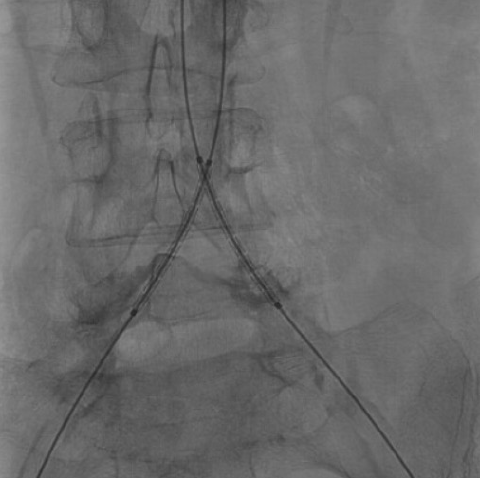
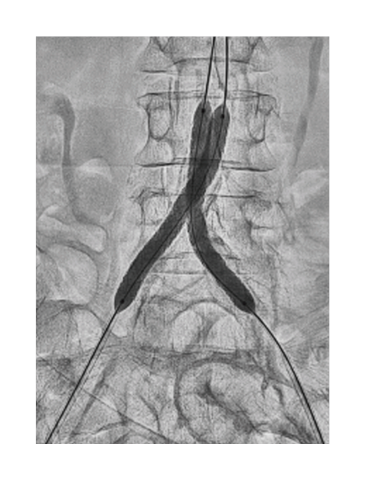
Figure 2. Positioning of kissing bilateral VBX Stent Graft.

Figure 3. Post-deployment angiogram.
Result
- Post-procedure follow-up revealed resolution of claudication symptoms. Right ABI = 1.01, Left ABI = 0.98.
- At six-year follow-up, patient remained asymptomatic with normal ABI bilaterally (Figure 4).
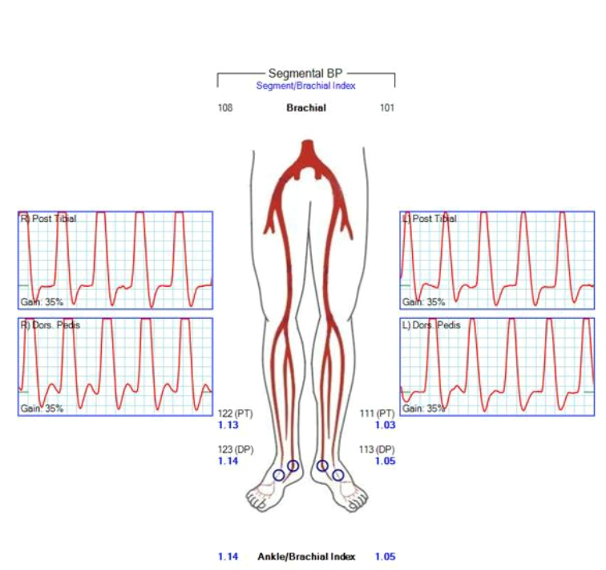
Figure 4. Six-year follow-up ABI. Left = 1.05, Right = 1.14.
Case takeaways
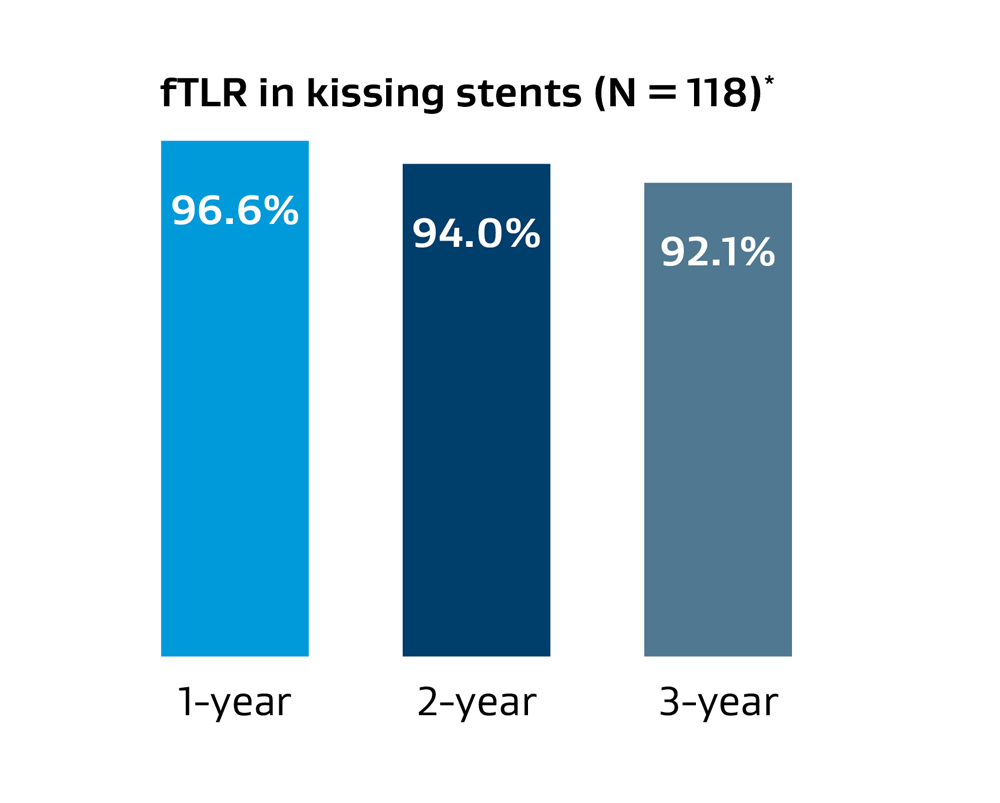
Complex AIOD can be managed via endovascular means with sustained long-term clinical durability. The COBEST trial demonstrated the benefits of using covered stents over bare metal stents for TASC II C and D aortoiliac lesions.1 The Gore VBX FLEX Clinical Study evaluated the safety and effectiveness of the VBX Stent Graft for the treatment of AIOD with freedom from target lesion revascularization (fTLR) in kissing stents at one and three years, 96.6% and 92.1%, respectively.*
This case highlights the use of the VBX Stent Graft for the treatment of advanced calcific aortoiliac lesions as both safe and effective in appropriate patients with excellent long-term durability.
Images courtesy of Jean Panneton, M.D. Used with permission.
Restoring flow to a patient with stenosis at the aortoiliac bifurcation
GORE® VIABAHN® VBX Balloon Expandable Endoprosthesis
Case submitted by Masahiko Fujihara, M.D.
Osaka, Japan
Challenge
- 78-year-old female with severe intermittent claudication (Rutherford 3)
- Bilateral common iliac artery stenosis (TASC II D lesions) originating at the aortic bifurcation
- Relevant patient history:
- Hypertension, hyperlipidemia, prior bilateral carotid artery stenosis
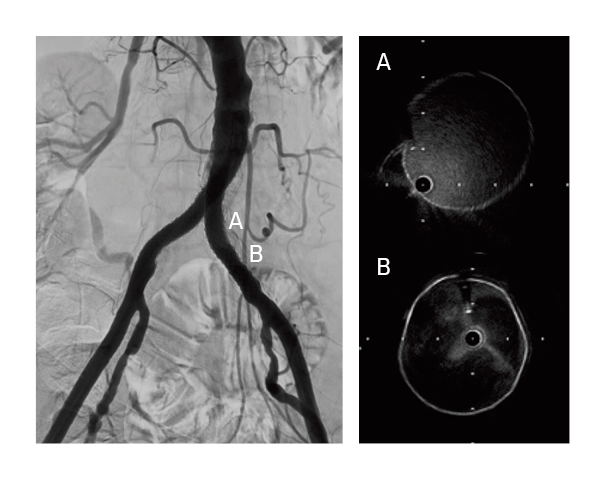
Calcified nodule at the aortoiliac bifurcation
Procedure
- Gained bilateral access in the common femoral arteries
- Crossed lesions on both the left and right with .014" guidewires
- Dilated with a 2 mm diameter percutaneous transluminal angioplasty (PTA) balloon to allow for intravascular ultrasound examination
- Pre-dilation with 5 mm balloons in kissing balloon technique
- Exchanged to .035" stiff guidewires and 7 Fr long sheaths
- Deployed two 7 mm x 79 mm GORE® VIABAHN® VBX Balloon Expandable Devices (VBX Stent Graft) using kissing stent technique
- Due to significant calcification, post-dilated first with two 8 mm x 40 mm PTA balloons
- Sequential post-dilation of VBX Stent Grafts proximally with a 10 mm x 20 mm PTA balloon followed by final post-dilation with kissing 8 mm x 40 mm PTA balloons
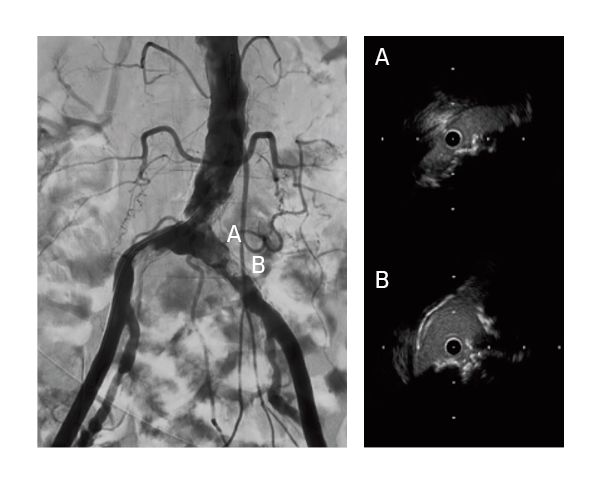
- Confirmed successful result using intravascular ultrasound and angiography
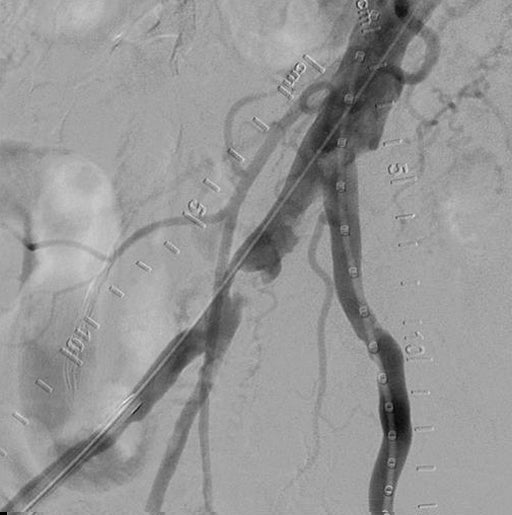
GORE® VIABAHN® VBX Balloon Expandable Endoprosthesis deployment
Final post-dilation of the GORE® VIABAHN® VBX Balloon Expandable Endoprosthesis
Result
- The patient was discharged with a full ankle-brachial index recovery and no remaining symptoms.
Fully expanded GORE® VIABAHN® VBX Balloon Expandable Endoprosthesis across the calcified segment
Case takeaways
The VBX Stent Graft provides durable outcomes in highly calcified lesions. The performance of the VBX Stent Graft allows device customization to the anatomy (6-11 mm for 7 mm x 79 mm device) and provides radial strength to achieve luminal gain while potentially mitigating the risk of rupture and perforation.
Images courtesy of Masahiko Fujihara, M.D. Used with permission.
Restoring flow in a patient with severe claudication and focal iliac calcification
GORE® VIABAHN® VBX Balloon Expandable Endoprosthesis
Case submitted by Chris Metzger, M.D.
Kingsport, Tennessee
Challenge
- A 57-year-old male with severe intermittent claudication (Rutherford 3).
- TASC II B lesion in the right common iliac artery (CIA) and focal iliac calcification.
- Relevant patient history:
- Current smoker with hypertension, hyperlipidemia and previous diagnosis of peripheral artery disease in the right limb that was treated with medication.
- Baseline ankle-brachial index (ABI) = 0.76.
Focal calcification in the right CIA
Procedure
- Started with bilateral access, identified focal lesion in the distal right CIA that was ~80% stenosed.
- Angiography showed robust multi-vessel distal runoff down to the foot.
- Pre-dilated with a 5 × 20 mm ABBOTT® ARMADA PTA balloon, observed presence of calcification nodule that prevented full dilatation of the percutaneous transluminal angioplasty (PTA) balloon.
- Delivered and deployed an 8 mm × 39 mm GORE® VIABAHN® VBX Balloon Expandable Endoprosthesis (VBX Stent Graft).
- Slight residual stenosis observed following VBX Stent Graft deployment.
- Post-dilatation performed using a 7 × 20 mm ABBOTT® ARMADA PTA balloon inflated to 14 atm (near rated burst pressure).
- Final angiogram showed complete restoration of patency in the right CIA with good distal outflow.

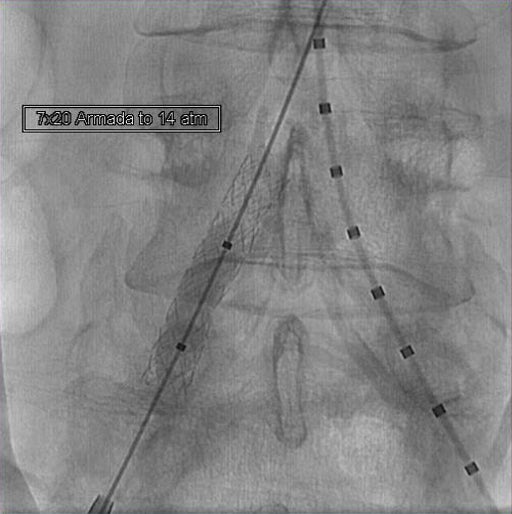
GORE® VIABAHN® VBX Balloon Expandable Endoprostheiss deployment and post-dilatation
Result
At discharge, the patient’s ABI was 1.0. At three-year follow-up, ABI was measured at 0.99 and patient was Rutherford 0 with no report of pain/discomfort or problems with mobility.

Complete restoration of patency
Case takeaways
Calcified lesions present challenges in endovascular treatment of aortoiliac occlusive disease, including an increased risk of rupture. The VBX Stent Graft provides a barrier that mitigates concerns about neointimal hyperplasia and provides high radial strength to restore patency in even the most calcified lesions.2
Images courtesy of Chris Metzger, M.D. Used with permission.
* Data on file 2020; W. L. Gore & Associates, Inc; Flagstaff, AZ.
- Mwipatayi BP, Sharma S, Daneshmand A, et al; COBEST co-investigators. Durability of the balloon-expandable covered versus bare-metal stents in the Covered versus Balloon Expandable Stent Trial (COBEST) for the treatment of aortoiliac occlusive disease. Journal of Vascular Surgery 2016;64(1):83-94.e1.
- Bismuth J, Gray BH, Holden A, Metzger C, Panneton J; VBX FLEX Study Investigators. Pivotal study of a next-generation balloon-expandable stent-graft for treatment of iliac occlusive disease. Journal of Endovascular Therapy 2017;24(5):629-637.
22642555-EN