Restoring flow in a patient with severe claudication and focal iliac calcification
Case submitted by Chris Metzger, M.D.
Kingsport, Tennessee

Challenge:
- A 57-year-old male with severe intermittent claudication (Rutherford 3).
- TASC II B lesion in the right common iliac artery (CIA) and focal iliac calcification.
- Relevant patient history:
- Current smoker with hypertension, hyperlipidemia and previous diagnosis of peripheral artery disease in the right limb that was treated with medication.
- Baseline ankle-brachial index (ABI) = 0.76.
Focal calcification in the right CIA
Procedure:
- Started with bilateral access, identified focal lesion in the distal right CIA that was ~80% stenosed.
- Angiography showed robust multi-vessel distal runoff down to the foot.
- Pre-dilated with a 5 × 20 mm ABBOTT® ARMADA PTA balloon, observed presence of calcification nodule that prevented full dilatation of the percutaneous transluminal angioplasty (PTA) balloon.
- Delivered and deployed an 8 mm × 39 mm GORE® VIABAHN® VBX Balloon Expandable Endoprosthesis (VBX Stent Graft).
- Slight residual stenosis observed following VBX Stent Graft deployment.
- Post-dilatation performed using a 7 × 20 mm ABBOTT® ARMADA PTA balloon inflated to 14 atm (near rated burst pressure).
- Final angiogram showed complete restoration of patency in the right CIA with good distal outflow.


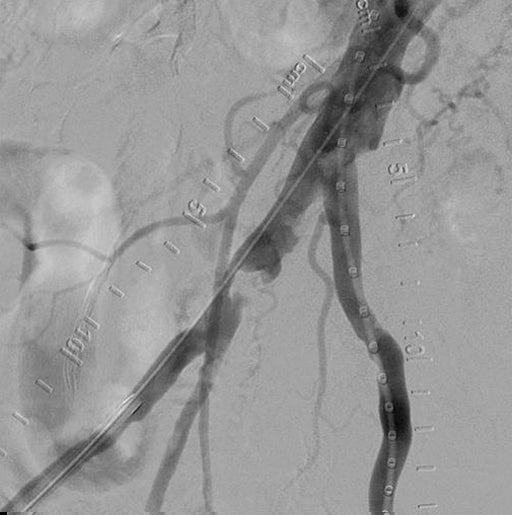
GORE® VIABAHN® VBX Balloon Expandable Endoprostheiss deployment and post dilatation
Result:
At discharge, the patient’s ABI was 1.0. At three-year follow-up, ABI was measured at 0.99 and patient was Rutherford 0 with no report of pain/discomfort or problems with mobility.

Complete restoration of patency
Case takeaways:
Calcified lesions present challenges in endovascular treatment of aortoiliac occlusive disease, including an increased risk of rupture. The VBX Stent Graft provides a barrier that mitigates concerns about neointimal hyperplasia and provides high radial strength to restore patency in even the most calcified lesions.1
Images courtesy of Chris Metzger, M.D. Used with permission.
- Bismuth J, Gray BH, Holden A, Metzger C, Panneton J; VBX FLEX Study Investigators. Pivotal study of a next-generation balloon-expandable stent-graft for treatment of iliac occlusive disease. Journal of Endovascular Therapy 2017;24(5):629-637.