Looking at the full scope of PAD: Cases, techniques, and economic considerations for complex disease.
Treatment Challenges for Femoropopliteal Lesions
Discussion on managing complex peripheral artery disease, particularly in the femoropopliteal region, and a relevant case study to highlight specific challenges.
WITH M. CASEY BECKER, MD, FACC, FSCAI, FSVM
Treatment Approach
With the complexities associated with peripheral artery disease (PAD), there is not an agreed upon modernday treatment algorithm. Given the multitude of PAD treatment options available, how do you make sense of it all?
Dr. Becker: It is very important to factor in individual patient characteristics, both anatomic as well as clinical, when deciding the appropriate intervention to perform. I remain very committed to data-driven intervention, and I think that each year we gain more evidence supporting our interventions. Despite that, there is still great latitude in decision-making and gaps in evidence for a specific approach. Knowledge of the data and experience with multiple device techniques is paramount to tailor the therapy to a specific patient. Although it may be tempting to apply drug-coated balloon (DCB) technology to all my patients, that is clearly not feasible and is not data driven. In light of the recent meta-analysis by Katsanos et al that suggests higher mortality with paclitaxel therapies,1 I am revamping my approach to these devices even more. It would be inappropriate to apply a certain standard size and type in most patients. A complete understanding of what the evidence shows and what it has failed to show, harmonized with good clinical experience and your own ability is key to patient care.
What does your algorithm look like when treating PAD?
Dr. Becker: Assuming that the least-invasive approach provides the patient with the highest chance of freedom from adverse events and the lowest risk, then I typically allow the lesion and anatomy to drive my PAD treatment algorithm. Therefore, after diagnostic imaging, the patient’s anatomy often dictates the best approach. For instance, short- to moderate-length lesions with low to moderate complexity are probably successfully treated with DCBs. However, as the lesion complexity increases, that probability drops linearly. It is at this point we need to convert our thinking toward the best stent technologies, where we actually have a wealth of data to help guide the proper device and placement technique. When it comes to the femoropopliteal location, vascular mimetic technology like the GORE® TIGRIS® Vascular Stent has become my primary choice due to the resistance of the forces on elongation, extension, torsion, and compression, as well as fracture resistance.
There has been a lot of discussion around the “leave-nothing-behind” approach over the last few years. In what clinical situations is this approach not necessarily enough?
Dr. Becker: An ideal situation is one in which we can apply DCB therapy and leave nothing behind. However, as we have clearly seen over the past couple of years, and with more data emerging at every meeting, the more complex lesions tend to have a higher rate of bailout stenting. Furthermore, most operators have become rather adept at assessing a lesion and its anatomy and deciding when it is reasonably futile to attempt DCB as a standalone therapy. It is in these situations, which are very common in clinical practice, that stent technology remains the primary endovascular tool. Then the question becomes: which stent performs best in this lesion subset and anatomic location? The GORE TIGRIS Vascular Stent delivers precise placement and expansion with optimal deployment in very challenging femoral popliteal lesions with excellent safety and efficacy data.
What unique challenges does treatment of a proximal popliteal lesion present?
Dr. Becker: The femoropopliteal segment remains the most hostile arterial bed in the body. Much biomedical engineering work has gone into characterizing the multiple reasons that this area has a high rate of arterial sclerosis and still remains quite hostile to endovascular therapy. The variation in sheer stress at this location combined with the extreme degrees of flexion, elongation, and tortuosity lead to a high degree of calcific arterial sclerosis. These factors make placement of most bare-metal stents (BMSs) extraordinarily challenging, which has been seen in multiple meta-analyses of trials involving BMSs at this location.2 The GORE TIGRIS Vascular Stent, however, was purpose-built to hold up in this environment and has demonstrated fewer fractures than any other commercially available device out there. It is also noted that the GORE TIGRIS Vascular Stent showed no elongation and zero stent fractures with excellent safety and efficacy in this particular zone.3
Device Selection
When you decide to stent, how do you choose which device to use?
Dr. Becker: If I am unable to perform successful DCB angioplasty (which may be a decision I make prior to or after dissection, and/or if recoil mandates it), I look to the lesion characteristics and pathology to help me select the proper prosthesis. Very short focal dissections or areas of recoil can usually be easily treated with implantation of a short BMS. Likewise, DCBs have great application here. However, as you approach the distal third of the superficial femoral artery (SFA) and enter the popliteal artery, data become more limited. What we know for sure is that traditional selfexpanding BMSs have a very high rate of failure; so much so, that it has been rather taboo to revascularize the popliteal artery in that fashion. However, with the advent of vascular mimetic technology like the GORE TIGRIS Vascular Stent, we have shown that this is now a very successful strategy. When properly applying to the proximal popliteal, we have two vascular mimetic implant (VMI) technologies in the United States to utilize at this location: the GORE TIGRIS Vascular Stent and the ABBOTT® SUPERA® Peripheral Stent System. The strong advantage of the GORE TIGRIS Vascular Stent is that it is extremely simple to deploy, its size, and there is no elongation or compression. Many operators find deploying the ABBOTT SUPERA Peripheral Stent System in this location intimidating or are concerned about the stent elongation, which has the potential to impact the patency rates.
Do your device considerations change when you are treating more complex lesions?
Dr. Becker: With regard to the SFA, it remains very clear that long, complex, occluded, and calcified lesions have poor long-term patency rates with BMSs. Even though we have seen better progress with drug-eluting stents and DCBs, there remains a high degree of bailout stenting and/ or prosthesis failure in these most complex of lesions. In this lesion subset, the GORE® VIABAHN® Endoprosthesis continues to demonstrate excellent results and safety.4,5 Therefore, when I approach a moderate to complex lesion, if I deem it not feasible to treat with DCB technology or I have the need for bailout stenting afterword, the GORE VIABAHN Endoprosthesis remains my first choice to revascularize these lesions. The robust dataset behind the stent as well as my personal clinical experience gives me great confidence in that strategy.
Case Report
An 82-year-old Caucasian male with claudication was referred to our service by his primary care provider due to nonhealing wounds involving the first three digits of his right foot. Further review of his medical history showed long-standing diabetes mellitus treated with insulin therapy, hypertension, hyperlipidemia, and coronary artery disease with two previous stent implantations. Although it was reported that the patient had stable claudication symptoms at 75 feet of ambulation, 7 weeks prior to presentation, the patient noted the eruption of ulceration on the aforementioned digits. At that time, the patient had been initiated on statin therapy, 325 mg of aspirin, and 50 mg of cilostazol twice daily. Despite referral to his local wound care clinic, the patient’s lesions continued to progress, and he was referred to specialty care.
Initial clinical inspection revealed clear evidence of arterial insufficiency involving digits one through three on the right foot. Femoral pulses were 2+ bilaterally; however, the popliteal pulse on the right was markedly diminished. Ankle-brachial indices (ABI) were 0.51 on the right (anterior tibialis) and 0.72 on the left. Pulse volume recordings showed markedly diminished amplitude and blunting of the waveforms at the level of the right anterior tibialis. Given the patient’s elevated creatinine at 2.13 mg/dL, it was decided to proceed to diagnostic aortography with lower extremity runoff and forgo CT angiography.
WHEN I APPROACH A MODERATE TO COMPLEX LESION, IF I DEEM IT NOT FEASIBLE TO TREAT WITH DCB TECHNOLOGY OR I HAVE THE NEED FOR BAILOUT STENTING AFTERWORD, THE GORE VIABAHN ENDOPROSTHESIS REMAINS MY FIRST CHOICE TO REVASCULARIZE THESE LESIONS.
Angiography revealed severe diffuse disease involving the distal third of the SFA becoming a total occlusion at the P1 segment of the popliteal artery (Figure 1). Reconstitution via genicular collaterals at the level of the distal tibioperoneal trunk was evident. The anterior tibialis had moderate diffuse disease, the peroneal artery was unaffected, and the posterior tibialis was totally occluded (Figure 2). A 6- X 45-cm destination sheath was taken across to the right common femoral artery. Unfractionated heparin was given to achieve an activated clotting time > 250 seconds. An ABBOTT® TREK® Coronary Balloon System and a TERUMO® GLIDEWIRE® ADVANTAGE Guidewire were used to navigate to the level of occlusion in the distal SFA.

Figure 2. Two-vessel tibial runoff noted after reconstituting the artery.

Figure 1. Severe TASC-D lesion of the distal SFA extending into the P2 segment.
At this point, a 0.035-inch SPECTRANETICS® QUICKCROSS Support Catheter was used to support a 0.014- inch ABBOTT® HI-TORQUE COMMAND Peripheral Guidewire to traverse the occlusion through small micro channels that were evident. Achieving luminal purchase in the anterior tibialis, an exchange was made for an 0.014-inch VASCULAR PERSPECTIVES ASAHI Grand Slam Guidewire and laser atherectomy was performed with a 2-mm SPECTRANETICS® TURBO-ELITE Laser Atherectomy Catheter at 40/25 fluency/rate; a second pass was made at 60/60 fluency/rate (Figure 3).
Vessel predilation was performed with a 5- X 100-mm SPECTRANETICS® ANGIOSCUPLT® PTA Scoring Balloon Catheter achieving full expansion at 12 ATM for 90 seconds. The P2-3 segment was then treated with a 5- X 80-mm SPECTRANETICS® STELLAREX Drug-Coated Angioplasty Balloon to 12 ATM for 2 minutes (Figure 4).
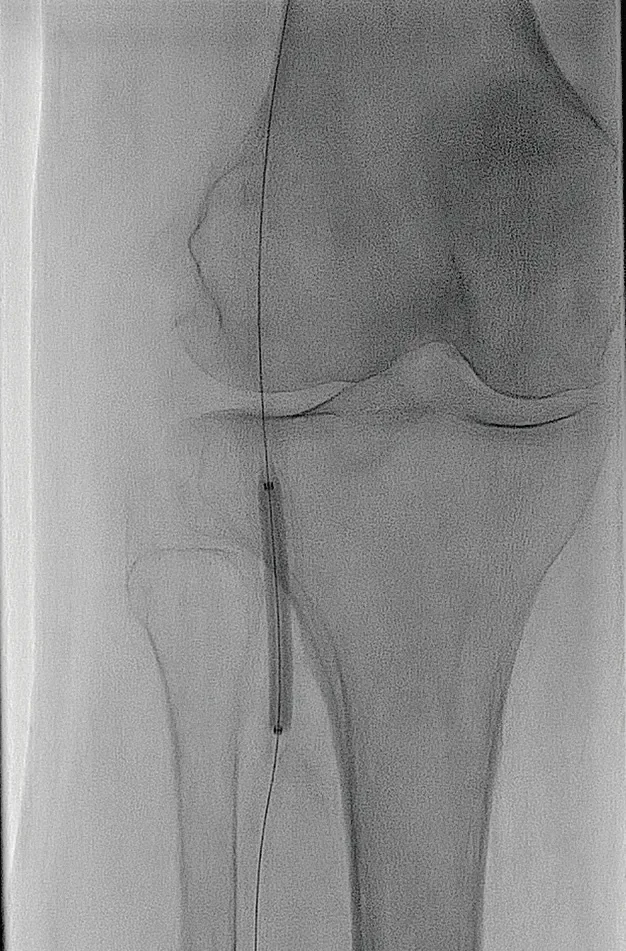
Figure 4. DCB therapy to the distal popliteal and tibioperoneal trunk.

Figure 3. Result after laser atherectomy with a 2-mm SPECTRANETICS® TURBO-ELITE Laser Atherectomy Catheter.
Following this, angiography confirmed an area of dissection and acute recoil in the P1 and P2 segments of the popliteal artery (Figure 5). Therefore, it was deemed unlikely that the DCB result would yield satisfactory long-term results and, therefore, endovascular scaffolding with a prosthesis was deemed appropriate. Given the femoropopliteal location, VMIs provide the best option. An intravascular ultrasound (IVUS) probe was passed throughout the length of the lesion and the distal reference vessel diameter was deemed to be 5 mm. Therefore, a 5- X 100-mm GORE TIGRIS Vascular Stent was implanted from the distal P2 segment into the distal SFA across the adductor hiatus (Figure 6).
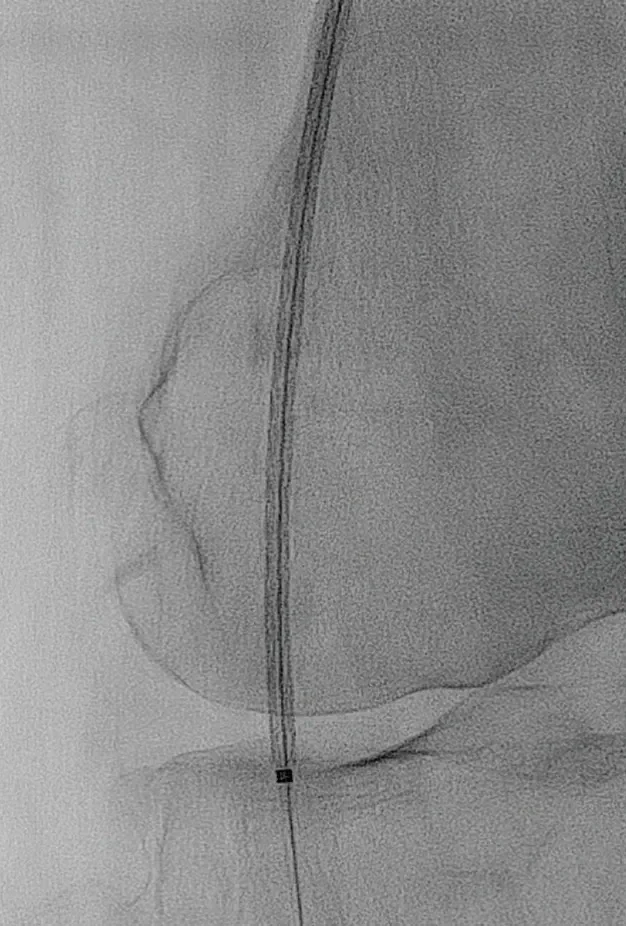
Figure 6. Precision placement of the GORE® TIGRIS® Vascular Stent to the P2 segment and across the adductor hiatus.

Figure 5. Predilatation shows extensive dissection, making successful DCB treatment unlikely.
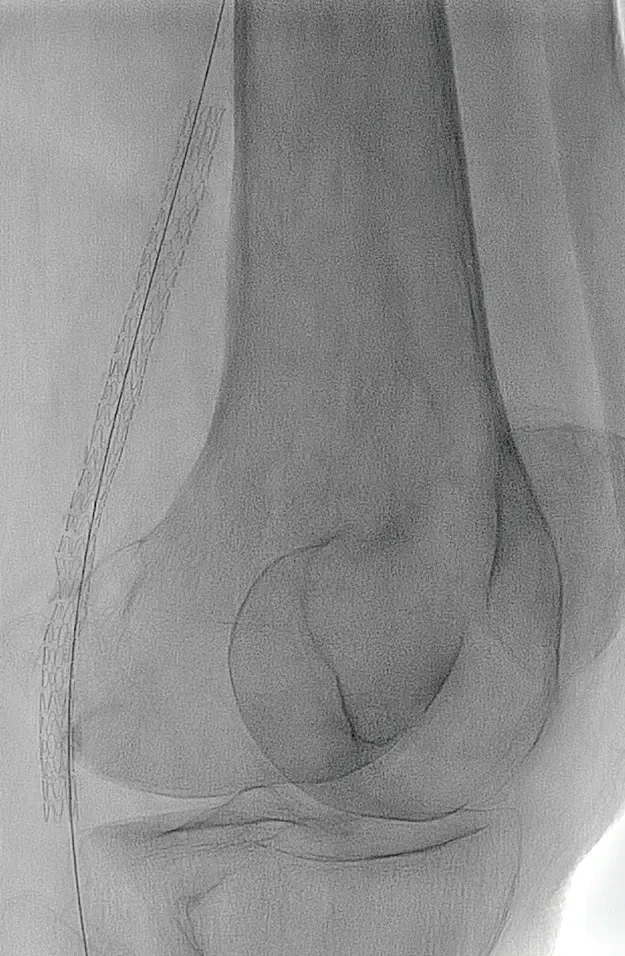
Figure 7. GORE® TIGRIS® Vascular Stent precisely deployed across the adductor hiatus without any elongation or fore shortening.
Postdilation was gently performed with a 5- X 100-mm ABBOTT TREK Coronary Balloon System. Final angiographic imaging showed excellent stent placement and expansion (Figure 7). Active flexation of the joint showed the stent to flex and rotate mimicking the natural arterial anatomy (Figure 8). Excellent tibial outflow to the angiosome of the import was confirmed (Figure 9). The patient was administered 300 mg of clopidogrel and continued on 81 mg of aspirin. Three-month follow-up in the wound clinic revealed an ABI of 0.91 (anterior tibialis) and total resolution of the ischemic lesions.

Figure 9. Improved twovessel tibial runoff at case completion.
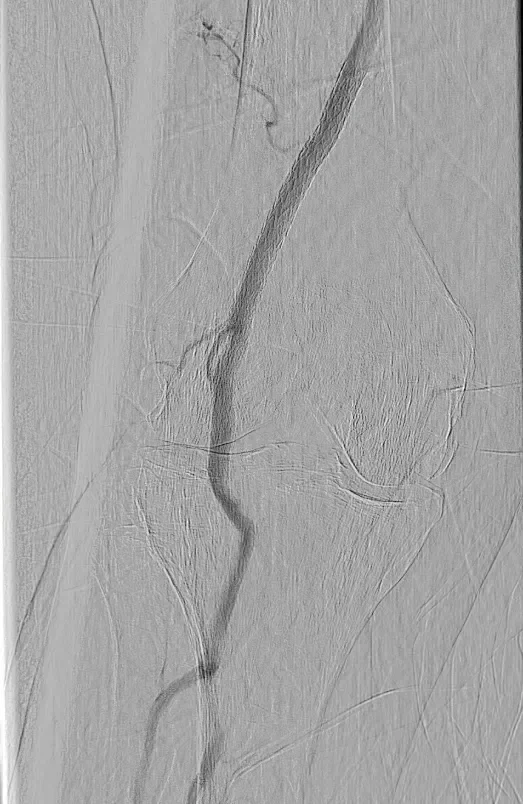
Figure 8. Active flexion of the knee joint shows resistance to kinking.
Discussion
The femoropopliteal arterial expanse has long posed a challenge for endovascular therapies. The notable presence of vessel tortuosity and curvature results in nonlaminar flow, mechanical strain, and a high variation in shear stress, which predispose to atherosclerosis and restenosis.6 Fracture of nitinol self-expanding BMSs is commonplace in this location, resulting in poor patency rates of 55% to 65% after 1 year, thereby limiting their efficacy in this position.7,8 VMIs, unique in their design and ability to conform to the vessel through highly malleable nitinol configuration, are better equipped to resist the flexion, extension, compression, and torsion of the femoropopliteal segment.9 Not surprisingly, this translates to improved patency rates, freedom from fracture, and better long-term outcomes.
Figure 10. GORE® TIGRIS® Vascular Stent.
In the current United States marketplace, two VMIs predominate: the GORE TIGRIS Vascular Stent and ABBOTT SUPERA Peripheral Stent System. The GORE TIGRIS Vascular Stent utilizes two components: nitinol stent rings that are coated with expanded polytetrafluoroethylene and a fluoropolymer interconnecting structure with a heparin bioactive surface (Figure 10). The GORE TIGRIS Vascular Stent is designed to conform to the anatomy and allow vessel movement, minimize fracture risk, and permit axial compression while resisting stent elongation. Results of studies evaluating the GORE TIGRIS Vascular Stent in diverse populations show 90% freedom from target lesion revascularization (TLR) at 12 months in shorter lesions,10 and 86% freedom from TLR at 12 months in a more highrisk population.11 Despite complex lesion characteristics, the GORE TIGRIS Vascular Stent group had zero fractures at 3 years and no stent elongation as compared with the nitinol self-expanding BMS group, where fracture was documented in 28.8% of cases.3,12
Recent data from the SUPERB trial shows that at 2 and 3 years, freedom from clinically drive (CD)-TLR was 86.7% for minimal compression and 90.0% for moderate compression, respectively. In those stents deployed with minimal (10%–20%), moderate (20%-40%), or severe elongation (> 40%), freedom from CD-TLR was 84.1%, 87.4%, and 77.0% at 12 months, respectively. At 2 and 3 years, for those stents that had severe elongation freedom from CD-TLR was 63.4% and 42.3%, respectively. It is notable that only 36% of stents were able to be deployed within the nominal range.13,14 Therefore, although both prostheses offer excellent safety and efficacy, the GORE TIGRIS Vascular Stent and its ease of use often garners it more favor in my clinical practice.
In regard to the patient case described, the operator is faced with a complex lesion of the femoropopliteal region and must choose the best therapy. After crossing the lesion and performing diligent vessel preparation, it became clear that treatment with DCB would have a high likelihood of failure due to acute recoil and dissection—observed in upwards of 30% of TransAtlantic InterSociety Consensus (TASC) C-D lesions in this region.15 Therefore, selecting the most appropriate stent becomes paramount for longterm success. Clinical trials of VMIs have demonstrated high patency and low fracture rates, making them ideal for this scenario. Furthermore, utilizing IVUS to properly size the prosthesis and precisely cover all diseased segments may also lead to better clinical outcomes.16 Due to the implementation of innovative technology and improved operator experience, utilization of endovascular therapies as a first-line approach continues to rise in complex TASC C-D lesions of the SFA and popliteal arteries. A strong command of the clinical data and proper implant techniques associated with these devices is paramount.
Conclusion
The femoropopliteal region remains one of the most hostile vascular environments and presents unique challenges to endovascular therapy. It is important to have familiarity with contemporary VMI technology and proper implant techniques to optimize clinical outcome in this region. As demonstrated by this case, careful and rigorous endovascular technique complimented by IVUSguided deployment of the GORE TIGRIS Vascular Stent achieved excellent results.
- Katsanos K, Spiliopoulos S, Kitrou P, et al. Risk of death following application of paclitaxel-coated balloons and stents in the femoropopliteal artery of the leg: a systematic review and meta-analysis of randomized controlled trials. J Am Heart Assoc. 2018;7:e011245.
- Weinstock BS. Covered stents in the treatment of superficial femoral artery disease. Vasc Dis Manag. 2014;11:E76-E86.
- Sibé M, Kaladji A, Boirat C, et al. French multicenter experience with GORE TIGRIS Vascular Stent in superficial femoral and popliteal arteries. J Vasc Surg. 2017;65:1329-1335.
- Lammer J, Zeller T, Hausegger KA, et al. Sustained benefit at 2 years for covered stents versus bare-metal stents in long SFA lesions: the VIASTAR Trial. Cardiovasc Interv Radiol. 2015;38:25-32.
- Ohki T, Kichikawa K, Yokoi H, et al. Outcomes of the Japanese multicenter Viabahn trial of endovascular stent grafting for superficial femoral artery lesions. J Vasc Surg. 2017;66:130-142.e1.
- Schlager O, Zehetmayer S, Seidinger D, et al. Wall shear stress in the stented superficial femoral artery in peripheral arterial disease. Atherosclerosis. 2014;233:76–82.
- Werner, M. Factors affecting reduction in SFA stent fracture rates. Endovasc Today. 2014;13(10): 93-95.
- Bosiers M, Deloose K, Callaert J, et al. Results of the Protégé EverFlex 200-mm-long nitinol stent (ev3) in TASC C and D femoropopliteal lesions. J Vasc Surg. 2011;54:1042-1050.
- Arena FJ, Arena FA. Intravascular ultrasound evaluation of interwoven nitinol stents at implant. J Vasc Med Surg. 2013:1:116.
- Piorkowski M, Freitas B, Steiner S, et al. Twelve-month experience with the GORE TIGRIS vascular stent in the superficial femoral and popliteal arteries. J Cardiovasc Surg (Torino). 2015;56:89-95.
- Parthipun A, Diamantopoulos A, Kitrou P, et al. Use of a new hybrid heparin-bonded nitinol ring stent in the popliteal artery: procedural and mid-term clinical and anatomical outcomes. Cardiovasc Intervent Radiol. 2015;38:846-854.
- W. L. Gore & Associates, Inc. Evaluation of the GORE® TIGRIS® Vascular Stent in the treatment of atherosclerotic lesions of the superficial femoral and proximal popliteal arteries. [Final post-approval study report-executive summary]. Flagstaff, AZ: W. L. Gore & Associates, Inc; 2017. MD165299.
- Garcia LA, Rosenfield KR, Metzger CD, et al. SUPERB final 3-year outcomes using interwoven nitinol biomimetic Supera stent. Catheter Cardiovasc Interv. 2017;89:1259-1267.
- US Food and Drug Administration. Supera peripheral stent system: instructions for use. https://www.accessdata. fda.gov/cdrh_docs/pdf12/P120020c.pdf. Accessed January 22, 2019.
- Schmidt A, Piorkowski M, Görner H, et al. Drug-coated balloons for complex femoropopliteal lesions: 2-year results of a real-world registry. JACC: Cardiovasc Interv. 2016;9:715-724.
- Spark JI, Allan RB. IVUS for GORE TIGRIS vascular stent placement during knee flexion. 2018;17(2)(supp):19-22.

This product has been discontinued.

Endovascular Today February 2019 Supplement
Looking at the Full Scope of PAD

M. Casey Becker, MD, FACC, FSCAI, FSVM
Peripheral, Structural, and Coronary Interventional
Therapies Division
Saint Vincent Heart and Vascular Institute
President and Founder
Panvascular Consulting LLC
Erie, Pennsylvania
Disclosures: Consultant to Gore & Associates.